E-LOGS MEDICINE
Hi, I am Arefin Sadat, a final-year MBBS student. This is an E-Log that depicts the patient-centered approach to learning medicine. This E-Log has been created after taking consent from the patient and their relatives. The links that were used by me for understanding the available data on the particular disease have been mentioned below in each post. I hope you learn valuable information after giving it a good read.
November 15, 2022
29 Years Old Female with SLE and Avascular Necrosis of Hip
CHEIF COMPLAINTS :
29/F came to OPD with C/o Loss of appetite , weight since 2 years
Generalised weakness and easy fatiguability since 2 years .
C/o Fever since 6 months
C/o Multiple joint pains and swelling since 6 months
Difficulty in movements and walking since 6 months.
C/o Hyper-pigmented leisons over cheeck bones and chin ,ears , b/l fore arm since 4 months .
C/o Severe hair loss since 4 months .
HOPI AND PAST HISTORY :
NO H/o decreased urine output or frothy urine, red color urine.
NO H/o chest pain, shortness of breath ,PND.
NO H/o bluish ,white discoloration of limbs on exposure to cold .
No h/o dry eyes and dry mouth .
FAMILY HISTORY :
No family history of joint pains/ other auto-immune diseases.
Younger sister SCD .
EDUCATIONAL STATUS :
Patient completed her BA .
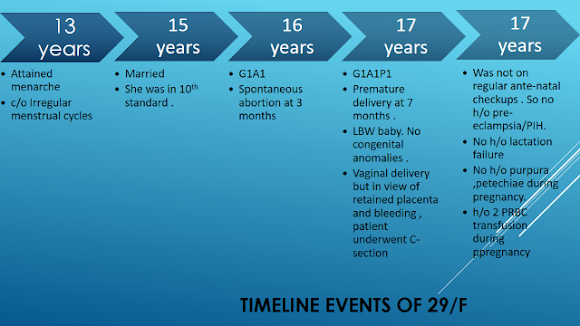
MARITAL HISTORY :
Married at 15 years of age . But divorced at 20 years of age.
SOCIAL HISTORY :
Poor socio-economic status .
PROVISIONAL DIAGNOSIS :
PROBLEM REPRESENTATION :
- H/o recurrent abortions , and young onset CVA , Seizures suggests ? HYPER-COAGULABLE STATE
-29/F with recurrent history of fever and multiple joint pains , rash and hair loss , loss of appetite and weight ,fatigue - all point towards auto immune etiology ,especially in a young female .
2-3 year history of bilaterally symmetrical ,chronic progressive inflammatory polyarthritis predominantly involving small joints .
Features favouring an inflammatory pathology are -
- Features of inflammation such as severe pain associated with edema of the joints and limitation of range of active movements
- Early morning stiffness, lasting for more than 30 mins (for 1 hour in this patient)
- Pain and edema of joints improving with activity and worsening with rest
- Features of uncontrolled systemic inflammation such as fever, involuntary loss of weight associated with loss of appetite.
- Swellings at joints and deformation of normal joint posture
Provisional Diagnosis - Bilaterally Symmetric Chronic Progressive Inflammatory Peripheral Polyarthritis
GENERAL EXAMINATION :
Patient was conscious, coherent and co-operative .
In Supine Position
Pulse - 94 bpm, regular, normal volume, condition of vessel wall - normal, no radio-radial or radio-femoral delay. All peripheral pulses were normal.
Blood Pressure - 110/80 mmHg - RIGHT ARM , supine posture .
110/70 mmhg -Left arm , supine posture .
Temperature - 99 F
Respiratory Rate - 18 cycles per minute , thoraco-abdominal type , no usuage of accesory muscles .
BMI - 18.3
JVP - Not elevated .
Pallor - present
No icterus ,clubbing ,cyanosis , lymphadenopathy ,edema .
Head to Toe General Examination
GENERAL CONDITION - Lean and thin built
HAIR - Thinning of hair noted on scalp . Non scarring alopecia present .
EYES - No conjunctival chemosis or injection, No redness or corneal lesions. Palpebral conjunctival pallor +. No icterus.
SKIN - Multiple, hyper-pigmented, well defined plaque/macules noted over face ,ears and fore-arm.
ORAL CAVITY - No ulcers currently
FINGERS AND NAILS - No clubbing or cyanosis , pallor -
GENERAL HEAD NECK AND ENT EXAMINATION - No abnormalities. No lymph node enlargement.
AXIAL - No apparent spinal deformities
Systemic Examination
Musculo-Skeletal System :
Axial Skeleton
Inspection - No visibly apparent spinal deformities;
Palpation - Inspectory findings confirmed. No spine tenderness.
Movements -
CERVICAL SPINE - Atlanto-occipital - Flexion, extension and lateral flexion normal .
Atlanto-axial - Rotation of head normal
FLESCHE TEST - Occiput to wall distance is zero - normal
THORACIC SPINE - Flexion , extension ,lateral bending , rotation - normal
SCHOBER'S TEST - normal
STRAIGHT LEG RAISING TEST (SLRT) - Pain present in hip joint . Not in back
SACRO-ILIAC JOINT - DIRECT PRESSURE - No pain
PATRICK'S TEST - no pain
GAENSLEN'S TEST - no pain
APPENDICULAR SKELETON :
UPPER LIMBS :
JOINTS | RIGHT | LEFT |
1)SHOULDER JOINT a) Inspection : Attitude of limbs – Swelling – Skin - Deformity – Muscle wasting – b)Palpation : Tenderness – Warmth – Synovial thickening – Crepitus – c) Range of movements : Active Passive | Slightly flexed and internally rotated; Contour normal NO NO ERYTHEMA NO NO All inspiratory findings confirmed YES NO NO NO Slight limitation of active and passive extension and overhead abduction | Slightly flexed and internally rotated; Contour normal NO NO ERYTHEMA NO NO All inspiratory findings confirmed YES NO NO NO Slight limitation of active and passive extension and overhead abduction |
2)ELBOW JOINT a) Inspection : Attitude of limbs – Swelling – Skin - Deformity – Muscle wasting – b)Palpation : Tenderness – Warmth – Synovial thickening – Crepitus – c) Range of movements : Active Passive | Attitude - mid-flexion; alignment of elbow and forearm - normal; YES NO erythema No No YES SLIGHT NO NO No restriction | Attitude - mid-flexion; alignment of elbow and forearm - normal; NO NO erythema No No YES NO NO NO No restriction |
3)WRIST JOINT: a) Inspection : Attitude of limbs – Swelling – Skin - Deformity – Muscle wasting – b)Palpation : Tenderness – Warmth – Synovial thickening – Crepitus – c) Range of movements : Active Passive | MILD EXTENSION No No No No Yes No No No Limitation of active and passive ulnar deviation | MILD EXTENSION No No No No Yes No No No Limitation of active and passive ulnar deviation |
4)HANDS (small joints) a) Inspection : Attitude of limbs – Swelling – Skin - Deformity – Muscle wasting – b)Palpation : Tenderness – Warmth – Synovial thickening – Crepitus – c) Range of movements : Active Passive | Fingers flexed at MCP and PIP MILD NO ERYTHEMA NO NO Present at MCP,PIP NO NO NO Slight Limitation of passive flexion at MCP | Fingers flexed at MCP and PIP MILD NO ERYTHEMA NO NO Present at MCP,PIP NO NO NO Slight Limitation of passive flexion at MCP |
5)HIP JOINT : a) Inspection : Attitude of limbs – Swelling – Skin - Deformity – Muscle wasting – b)Palpation : Tenderness – Warmth – Synovial thickening – Crepitus – c) Range of movements : Active Passive | Slight flexed and internal rotated NO NO erythema No No Yes No No No Limitation of passive and active movements of flexion and extension. (towards the end of range of motion); | Slight flexed and internal rotated NO NO erythema No No Yes No No No Limitation of passive and active movements of flexion and extension( towards the end of range of motion); |
6) KNEE JOINT : a) Inspection : Attitude of limbs – Swelling – Skin - Deformity – Muscle wasting – b)Palpation : Tenderness – Warmth – Synovial thickening – Crepitus – c) Range of movements : Active Passive | MILD NO erythema No No Yes No No No No restriction | MILD NO erythema No No Yes No No No No restriction |
7) ANKLE JOINT: a) Inspection : Attitude of limbs – Swelling – Skin - Deformity – Muscle wasting – b)Palpation : Tenderness – Warmth – Synovial thickening – Crepitus – c) Range of movements : Active Passive | Dorsiflexed Yes (minimal) No No No Yes Slight No No Limitation of passive and active plantar flexion | Dorsiflexed Yes No No No Yes Slight No No Limitation of passive and active plantar flexion |
8) FEET EXAMINATION : a) Inspection : Attitude of limbs – Swelling – Skin - Deformity – Muscle wasting – b)Palpation : Tenderness – Warmth – Synovial thickening – Crepitus – c) Range of movements : Active Passive | Foot hanging on side of bed No No No No Yes at MTP,PIP NO No No Limitation of passive movements of flexion and extension of MTP joints | Foot hanging on side of bed No No No No Yes at MTP ,PIP NO No No Limitation of passive movements of flexion and extension of MTP joints |
| | |
| | |
OTHER SYSTEM EXAMINATION :
Cardiovascular System - No abnormalities detected
Respiratory System - No abnormalities detected
Abdominal Exam - No abnormalities detected
Nervous System -NO abnormalities detected.
SCHOBERS TEST :
Examination Video links :
INVESTIGATIONS :
Serum LDH:- 212 IU/L
Random blood sugar :- 85mg/dl
COMPLETE BLOOD PICTURE :-
Hb:- 7.3%
TLC:- 6,400
Neutrophils :- 67%
Lymphocytes :- 30%
Monocytes :- 2%
Eosinophils:- 1%
PCV:-22.4%
MCV:- 80.3
MCH:- 26.2
MCHC:- 32.6
RBC:- 2.79 million/cumm
PLATELETS:- 1.16 lakhs
NC/NC - PICTURE .
DCT- POSITIVE
COMPLETE URINE EXAMINATION:-
Pus cells- 4-5
Epithelial cells :- 2-3
Albumin :- 2+
Sugars :- Nil
No RBC
Urine protein/ Creatinine ratio:-
Spot urine protein:- 10 mg/dl
Spot urine creatinine:- 171.2 mg/dl
Ratio:- 0.05
RFT :-
Urea:- 34 mg/dl
Creatinine:- 0.9 mg/dl
Uric acid :- 5.3 mg/dl
Calcium:- 10.1 mg/dl
Phosphorus :- 3.7 mg/dl
Sodium:- 139 mEq/L
Potassium:- 3.5 mEq/L
Chloride :- 98 mEq/L
LFT:-
Total Bilirubin :- 0.51 mg/dl
Direct Bilirubin:- 0.16 mg/dl
AST:- 18 IU/L
ALT:- 10 IU/L
Alkaline phosphatase:- 98 IU/L
Total proteins :- 5.6 gm/dl
Albumin :- 3.2 gm/dl
A/G ratio:- 1.17
Serology :- NEGATIVE
ULTRASOUND
Impression :-
1) Mild splenomegaly
2) Mild Ascites
3) Hemorrhagic cysts in right ovary
2D ECHO:-
Impression:-
EF:- 56%
RVSP:- 30mmhg
TRIVIAL TR+/ AR+, No MR
NO RWMA , NO AS/MS
Good LV Systolic Functions
No diastolic Dysfunctions ,
NO PAH/PE
Previous admission fever chart :
FINAL DIAGNOSIS :
The patient has Fever , fatigue ,hyper-pigmented rash on malar surface ,loss of appetite ,non scarring alopecia and
Bilaterally Symmetrical Chronic , Non erosive peripheral Polyarthritis, predominantly involving small joints with pain ,tenderness , early morning stiffness and swelling ,and restricted movemets .
Differential diagnosis for such conditions include - 1) SLE
2) MCTD
3) Polymyositis and dermatomyositis
4) Rheumatoid arthritis - but its erosive
5) Systemic sclerosis
In background of strong ANA positivity, anti- ds-DNA ,anti- smith , anti ro antibodies
, SLICC criteria more than 4
SLE is likely diagnosis- with skin ,joint , CNS lupus , anemia of chronic disease and thrombocytopenia.
? Associated with APLA - in view of recurrent abortion history and CVA
? Moderate Depression ( Score 18 - according to Hamilton-depression score )
TREATMENT :
1) TAB PREDNISOLONE 20 MG BD
2) TAB HCQ 200MG BD
3) TAB ACECLOFENAC 100MG BD
4) TAB DOLO 650 MG SOS
5) TAB PANTOPRAZOLE 40 MG OD
6) FUSIDIC CREAM LOCAL APPLICATION
FURTHER PLAN -
SLE is a life long disease ,and balance has to be maintained always between infections and immunosuppression .
FLARE has to be prevented .
1) Screen for APLA
2) 24 HOUR URINE PROTEIN EXCRETION - If >1g/day - Plan for renal biopsy .
3) Start patient on immunosupressants and ecosprin and anti- epileptics back
4) Improve her quality of life by reducing pain and able to get back to work and earn.
5) Psychiatric evaulation and counselling for suicidal thoughts and excessive thoughts .
6) Repeat screening of anti-ds DNA ,C3,C4 to know disease progression .
DISCUSSION :
1) SLE PATHOGENESIS ?
2) JOINT INVOLVEMENT :
3) SLICC CRITERIA :
4) ANTIBODIES IN SLE :
5) Sensitivity and specificity of ANA and anti-dsDNA in the diagnosis of systemic lupus erythematosus:
P- Serum samples from HC, MMP and SLE patients, 100 in each group, were analyzed for the presence of ANA and anti-dsDNA, by indirect immunofluorescent assay .
I - Antibody profiles assesment
C - Comparison of anti ds DNA and ANA in sera of SLE patients and sera from healthy controls and multiple medical conditions.
O - When using HC sera for the diagnosis of SLE, the sensitivity of ANA at a titer of ≥ 1:80 and ≥ 1:160 was 98% and 90%, respectively, with specificity of 92% and 96%, respectively. The specificity decreased to 88% and 94%, respectively, when using sera from MMP patients. The specificity of anti-dsDNA was 100% and 97%, when using sera from HC and MMP patients, respectively.
ANA and anti-dsDNA gave high sensitivity and high specificity in patients with SLE, even when using MMP patient's sera as controls.
6) Efficacy of cognitive behavioural therapy for the treatment of chronic stress in patients with lupus erythematosus: a randomized controlled trial
P - 45 patients with lupus and high levels of daily stress were randomly assigned to a control group (CG) or a therapy group (TG)
I - Received cognitive behavioural therapy (CBT) which consisted of ten consecutive weekly sessions.
C - Control sle patients
O - We found a significant reduction in the level of depression, anxiety and daily stress in the TG compared to the CG and a significant improvement in QOL and somatic symptoms in the TG throughout the entire follow-up period.
7)Thrombocytopenia in SLE ?
Is associated with a worse prognosis and higher mortality from the disease.12,16,17 It has been linked with a severe disease course including neuropsychiatric disorders, renal involvement, hemolytic anemia and antiphospholipid syndrome.
The leading cause of death in the Reveille et al.20 study was infection.
In two large studies thrombocytopenia was the only independent predictor for mortality in SLE.
8)Differentiating infection vs lupus flare ?
In our recent study on Korean patients with lupus, CRP levels higher than 1.35 mg/dL indicated the presence of an infection with 100% sensitivity and 90% specificity
. Leukocyte count is elevated in SLE with infection, and remains unchanged or decreased in SLE with flare
Complement levels and anti-dsDNA antibody titer are changed only in SLE with flare, but the changes are usually not considerable at already abnormal levels.
Overall, CRP is the most critical marker in differentiating between infection and disease flare up in SLE. In a recent study, fever duration, anti-dsDNA antibody titers, and CRP were regarded as the most reliable markers to distinguish between infection and SLE activity
Jung JY, Suh CH. Infection in systemic lupus erythematosus, similarities, and differences with lupus flare. Korean J Intern Med. 2017;32(3):429-438. doi:10.3904/kjim.2016.234

































Comments
Post a Comment